How Hawaii Can Get Coronavirus Right In Twelve Steps
by Darragh C. O’Carroll M.D.
This paper has been peer reviewed and endorsed by
- Paul S.Pottinger M.D. — Professor of Medicine, Division of Allergy & Infectious Diseases, University of Washington
- Michael W. Schwartz M.D. — Robert H. Williams Endowed Chair, Professor of Medicine, Division of Metabolism, Endocrinology and Nutrition, University of Washington
- Karl Kaiyala PhD — Research associate professor (emeritus), Department of Oral Health Sciences, School of Dentistry, University of Washington
- Lee Altenberg PhD — Adj Full Professor of Information and Computer Sciences and Mathematics, University of Hawai’i at Mānoa, Member of HiPAM
- D. Kapono Chong-Hanssen M.D. — Medical Director; Ho`ola Lahui Hawai`i/Kaua`i Community Health Center
- David Derauf M.D. MPH — Physician and Director of Kokua Kalihi Valley, Honolulu, Hawai’i
- Jonathan Dworkin M.D. — Board Certified in Internal Medicine and Infectious Disease, Waimea, Hawai’i
- Lee Evslin M.D. — Board Certified Pediatrician, Former CEO of Wilcox Medical Center, Kapaa, Hawai’i
- Brent Tatsuno M.D. — Board Certified in Pulmonology and Critical Care, Honolulu, Hawaii
Nobody wanted to be suffering eight months into a global pandemic, but here we are. One silver lining about being this far along is that we know much more than when we began, and have the tools to outwit this coronavirus if deployed properly. We have learned on the international, national, and local scale that as soon as you disregard SARS-CoV-2, it will come roaring back. To keep Hawai’i afloat from both a public health and economic perspective, we must follow up-to-date scientific knowledge and research, because mass availability of vaccinations and hope of reprieve are still many months away. We can’t afford missteps — our lives and livelihoods depend upon it.
What this paper does is walk through, in twelve steps, how Hawaii’s current strategy to screen visitors and returning residents has gone starkly against international scientific consensus by
- Overestimating the efficacy of a one test surveillance system
AND
2. Underestimating the amount of virus in the United States
This paper strongly recommends that Hawaii’s economic and public health leaders reconvene to honestly examine the efficacy of a one-test protocol. As the department of health has previously recommended, we also recommend reinstating some length of quarantine for visitors and returning residents culminating with a second test, as deemed acceptable by all parties. To continue with a one-test plan is putting workers in the visitor industry, and the entire state, at an unacceptably high risk.
Let’s start with some fundamental statistics, taken directly from the CDC’s website.
1. Why SARS-CoV-2 Is Unlike Prior Coronaviruses: Asymptomatic & Pre-Symptomatic Spread

The first row is the rate of asymptomatic persons, or persons who contract this disease but never develop symptoms. 40 percent of all persons infected with coronavirus are asymptomatic and will interact with people, travel, and spread this virus unknowingly. You would think these asymptomatic persons would be very inefficient at spreading disease, but if you look at the second row, they aren’t. Asymptomatic persons are 75 percent as infectious as those who do have symptoms.
Furthermore, those who eventually do have symptoms are infectious several days before these symptoms begin, collectively known as pre-symptomatic persons. Combining asymptomatic and pre-symptomatic spread leads to the last very important number…
Unlike the prior human coronaviruses MERS and SARS that were more easily contained, at least 50 percent of infections are transferred before there is any hint of infection.
2. CONTAINMENT STRATEGIES
Because at least 50 percent of infections are transferred before there is any hint of infection, there are two pillars of prevention in island nations and states like Hawaii (in addition to contact tracing [digital], public health messaging, and the availability of isolation/quarantine areas).
- Mask use by all
- Containment of asymptomatic and pre-symptomatic persons
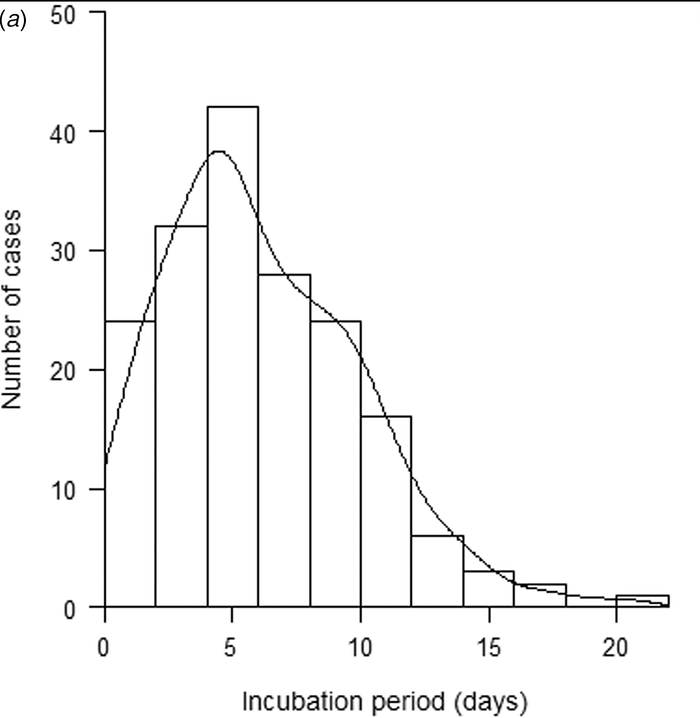
A fourteen day quarantine was Hawaii’s initial containment strategy, and a good one from a public health perspective, as after two weeks nearly everyone had passed their incubation period, or the number of days it takes to develop COVID-19 symptoms after exposure.
Below is an illustration of incubation periods, and it’s important to note that this period can be different for everyone. The length depends largely on the amount of virus encountered during exposure, but a commonly accepted average is 5–6 days, and rarely longer than fourteen.
Thus if a traveler has a negative test after fourteen days, it is 99% certain they will not be infectious to anyone else. Nations like New Zealand, Thailand, Hong Kong, Fiji, Australia, Taiwan and others continue to employ a fourteen day quarantine and release after a second negative test, especially if the traveler is from a high risk area.
Their residents and small businesses are enjoying lives and economic freedoms almost entirely unencumbered by this pandemic.
But for an economy like Hawaii’s that depends on high volume tourism, with an average length of stay dipping into the four day range during certain times of the year, continuing a fourteen day quarantine isn’t a tolerable option economically — we must strike a better public health and economic balance.
The solution to this dilemma, since May of 2020, has been one 72hr pre-arrival test.
3. HOW RELIABLE IS ONE TEST ?
The simple answer is that it depends on when the test is taken. Below is research from the Harvard School of Public Health released on June 27th. It depicts a concept called viral kinetics, or the amount of coronavirus inside a person over time — also called viral load. Focus on the viral load (black dotted line) and how it only appears on day 3, several days before symptoms begin.
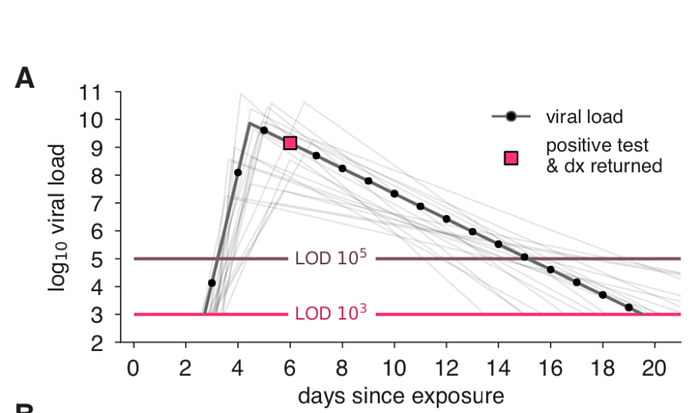
Much as it takes weeks for a pregnancy test to result positive, it also takes several days for the virus to grow to detectable levels. You can see that during the first three days of incubation, it doesn’t matter what test is used (pink and brown horizontal lines), the viral load is too low to detect.
4. FALSE NEGATIVE RATE OF OUR MOST SENSITIVE TESTS
On August 18th, the Annals of Internal Medicine released a seminal study on the false negative rate of our most sensitive PCR tests.
A false negative is a result that incorrectly indicates that the coronavirus is absent.
The red line has been added to reflect viral load, and it’s very clear during the first three days of incubation the probability of a false negative (black dots) is close to 100 percent. It means for the average person, a test on days one to three from exposure is not useful at all.
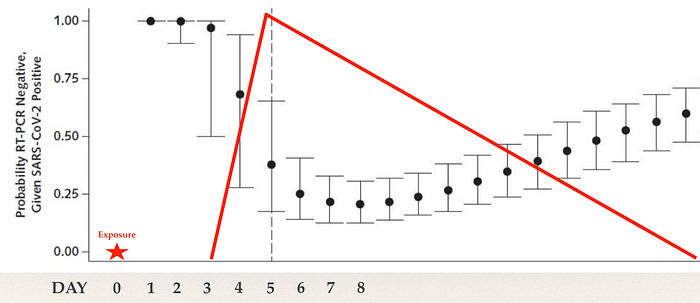
It’s only on day four of incubation that some notable efficacy is seen, where the false negative rate drops to about 65 percent. On Day five the false negative rate drops further to about 40 percent, and our tests peak in efficacy on day eight since exposure, with a 20 percent false negative rate.
5. GLOBAL CONSENSUS THAT ONE TEST IS NOT ENOUGH
What was just explained is a concept that is very widely accepted in the medical community, and why medical consultants to professional sporting organizations, the film industry, as well as nations who have controlled this virus use multiple tests AND a quarantine period to contain spread.
Below is a November 3rd release from CNN.

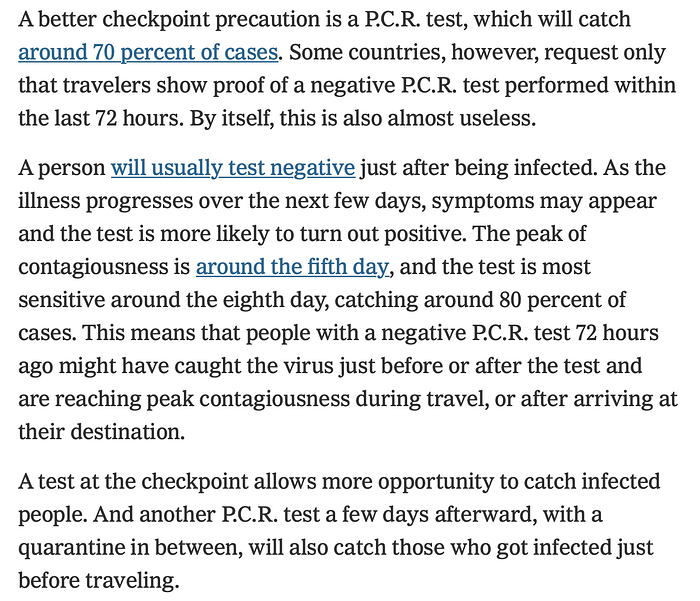
Next are a few paragraphs from a New York Times article released on September 14th, entitled “This is Why We Couldn’t Control the Pandemic”, by Tomas Pueyo.
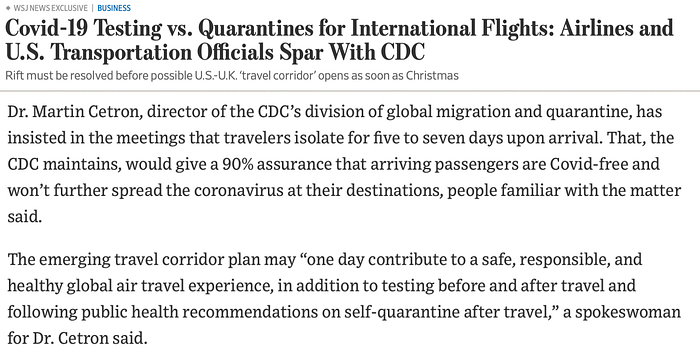
On October 19th the Wall Street Journal published recommendations of Dr. Martin Cetron, the CDC’s Director of global migration and quarantine, on the UK-USA travel corridor.
Lastly, on November 20th the Washington Post released this case study from New Zealand in which a traveler tested negative 48 hours prior to the flight, but became infectious and remained pre-symptomatic en route. The traveler eventually developed a fever 71 hours after arrival, but it led to a cluster of seven others, which would have continued to grow if not for New Zealand’s mandatory fourteen day quarantine.

6. SURVEILLANCE TESTING — It’s different than diagnostic testing.
So why are people recommending a second test? The New England Journal of Medicine published a letter on September 30th based on earlier work done by Harvard researchers, in which they advocate for increased testing frequency to control the spread of coronavirus.
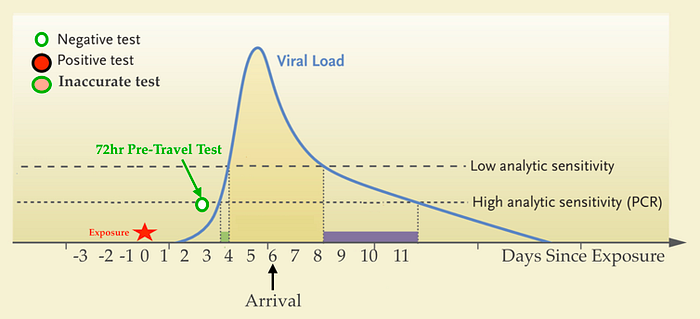
Below in blue is another depiction of viral load over time. Also included is the performance two types of tests:
1. Low sensitivity cheaper rapid tests
And
2. High sensitivity expensive PCR tests

The above picture demonstrates that because the viral load (in blue) increases so rapidly, using cheaper rapid tests more frequently will catch a greater number of infections than our expensive tests conducted sporadically.
This is called surveillance testing, and it’s very different from diagnostic testing.
The same Harvard researchers also published this in bar graph form, where they modeled several different surveillance strategies in a population of 10,000 people. The brown bars are cheaper lower sensitivity rapid tests, and the red bars are our expensive higher sensitivity PCR tests.
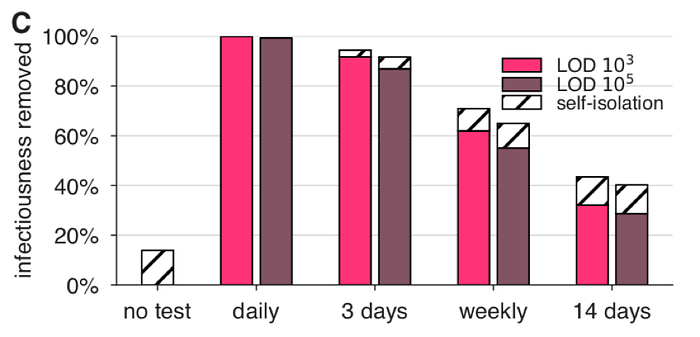
According to this Harvard model, if a surveillance test is conducted just once every fourteen days, which is similar to screening travelers with only one test, only 30 percent of asymptomatic and pre-symptomatic persons are caught. Just another 15 percent of persons will isolate themselves after developing symptoms (the dashed box on top).
United Healthcare group and Dr. Daniel Griffen of Columbia University Medical Center in New York released an interactive COVID-19 simulator in October that can calculate how effective any surveillance strategy is. Below is a screenshot after inputting a one test strategy, with the results highlighted in red.
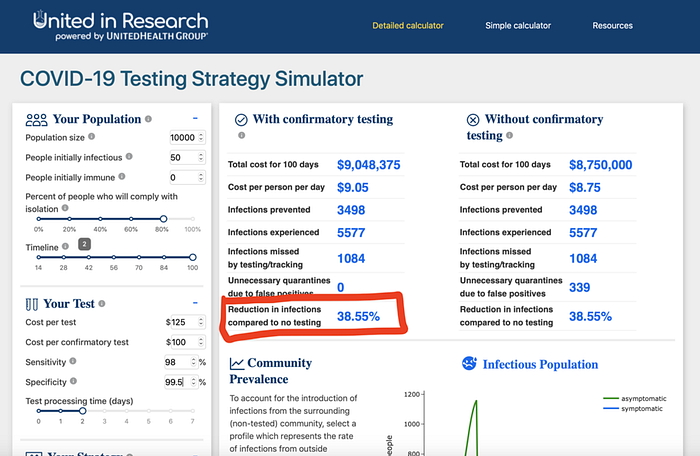
This COVID-19 simulator also depicts one test will catch less than 40 percent of infections. You can try it for yourself at the link here.
7. WHAT ARE OTHER COUNTRIES & STATES DOING?
The countries that have successfully controlled the spread of COVID-19 have instituted much stricter guidelines than Hawaii.
New Zealand, Australia, Taiwan, Thailand, Vietnam, Hong Kong, South Korea, Fiji, and Japan all have grading systems for how long an international visitor must quarantine. Their systems are based on infectious rates of the country of origin, but all place three countries in the VERY HIGH RISK category:
- The United States
- United Kingdom
- Brazil

The very low risk category requiring an entry test + no quarantine is reserved for travelers from countries like New Zealand, or places that have no active community spread.
The following figure is from a 93 page, 18 chapter, Australian paper entitled “The Transparent Risk Assessment of Quarantine” published in November by a multi-consortium of Australian universities, public health organizations, and endorsed by Qantas.
In it they found that a system like Hawaii’s, a no quarantine pre-test 3 days before arrival system (blue stars), will release 26x more infectious persons than a standard 14 day quarantine method (green star).

Putting it another way, Hawaii’s current system will again only catch roughly 40 percent of infectious persons.
8. What about the “Surveillance Testing” In Hawaii
Over 90% of what is currently being considered a surveillance test should be labelled as an entry test.
These entry tests can play a role, but are low sensitivity rapid antigen tests conducted on the same day, or close to the same day, as the pre-travel test at Hawaii Island’s airports.
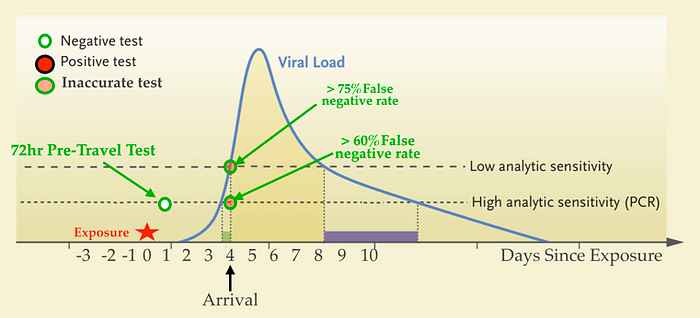
You can see below if an exposure occurs prior to departure (red star), and if the traveler opts for a rapid pre-test at the airport of origin, it’s very unlikely to flip positive after a 6–12 hour flight and subsequent entry test.
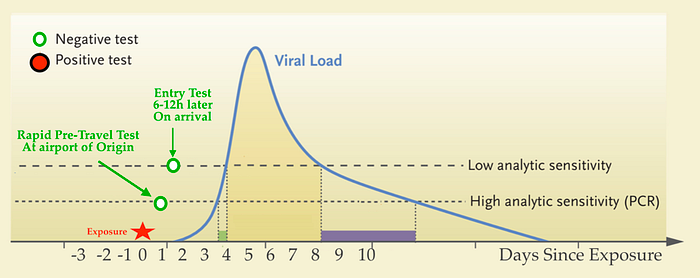
If an exposure occurred as far back as one day before the 72 hour pre-travel test, it’s still unlikely to flip positive on a subsequent entry test because rapid tests on day four post exposure have more than a 75 percent false negative rate.
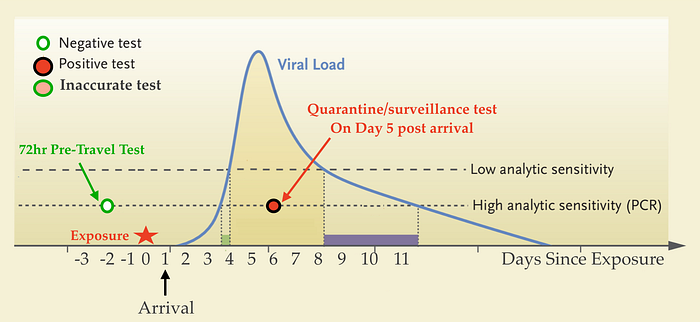
Thus, if you are only conducting one surveillance test for travelers, it will only begin to reflect true coronavirus rates if it’s a high sensitivity PCR test conducted somewhere closer to day 5 after arrival. A day 5 post arrival test would begin catching those exposed one day prior to travel, and the day of, but certaintly not all.
Our pacific neighbor, the Commonwealth of the Northern Mariana Islands, requires an entry test and a second test after 5 days of quarantine.
Again, it’s extremely inaccurate to classify entry tests as surveillance tests. Additionally if the surveillance test is voluntary, the result will be artificially low due to voluntary selection bias.
9. To Estimate the True Number of Infected Visitors Arriving to Hawaii, Look no further than Kauai
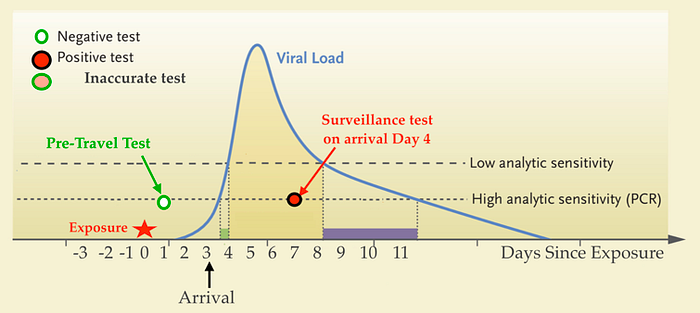
On Kauai all surveillance tests are done at minimum 4 days after arrival, which unlike entry tests, more frequently sit inside the window of a typical viral load curve. See Day 7 post exposure, or 4 days after arrival below.
From October 31st to November 18th, 5 of 331 visitors who tested negative prior to arrival on Kauai tested positive on day four of their vacation.
This is a positivity rate of 15 in 1000, a full 15x higher than the current program predicted.
Travel has been directly linked to a stark increase of infections on Kaua’i, which is no doubt seeding community spread on an island which has had none for months.

If it’s happening on Kauai, it’s happening on all of our islands. But the miscalculation can’t solely be explained by an overestimation of testing efficacy.
10. Prevalence — Estimating How Much Virus Is Out There
Another important number to know is prevalence, or how much virus is out there. A second oversight has occurred by drastically underestimating the true prevalence of disease in the United States, by only looking at case prevalence. Think of it as an Iceberg — the detected cases are just the visible tip.
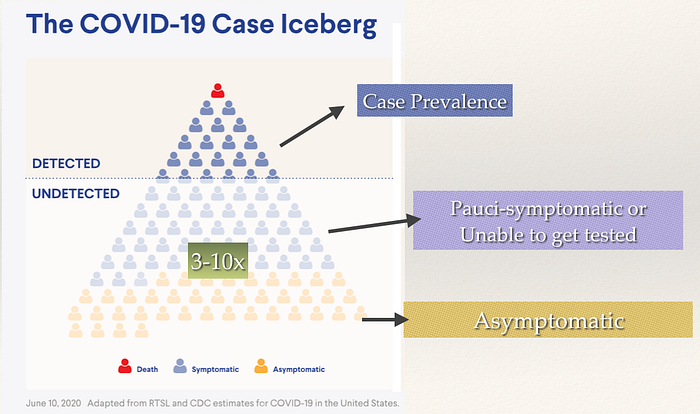
Case prevalence is the number of persons who tested positive and have active infection in a given area, it represents the number of active cases. This severely underestimates the true prevalence of disease in a community in several ways:
- A least 40 percent of infections are asymptomatic and unaware they carry this virus.
- Many people have symptoms that are so mild (pauci-symptomatic) they are also unaware they harbor coronavirus. It’s only after they incidentally test positive or are asked about symptoms, when they realize their extremely mild congestion, slight headache, mild diarrhea, or slight loss of smell was due to coronavirus.
- Many people are unable to be tested, don’t want to be tested, don’t believe in this virus, or fear the consequences of a positive test.
Because of the above, it’s very widely accepted that true prevalence is at least 3x higher than case prevalence, some estimates are as high as 10x.
HIPAM, a local data group here in Hawaii, estimates true prevalence by multiplying case prevalence by 7x.
When you combine the overestimation of testing accuracy by at least two-fold by neglecting viral kinetics, and underestimation of the true prevalence of this disease in the United States by a factor of 3x-10x, you get an infectious traveler rate that is at minimum 6x higher than estimated.
This is inline with international consensus, and explains Kauai’s results of 15 in 1000 positive visitors. A much more detailed analysis done by Karl Kaiyala PhD of the University of Washington can be found here.
11. Masks are Crucial, but so is a Fence
As cases continue to sky-rocket on the US mainland without an end in sight, it’s extremely clear one test is not enough to curb the influx of infectious visitors and returning residents, no matter what rate of mask use we achieve. See below how an asymptomatic or pauci-symptomatic traveler could be exposed 6 days prior to departure and arrive infectious to others by the current one-test system.
However, it’s undeniable that masks are also crucial to stop the spread of this coronavirus, and everyone should be using one!
Below in green is a prediction from the University of Washington Institute for Health Metrics and Evaluation regarding the decline in daily infections if mask use in Hawaii climbed from 80 percent, to 95 percent.

Masks are extremely important for everyone, especially indoors with extended family and friends outside of immediate bubbles. However, despite the clear evidence of mask efficacy, masks are taken off by visitors and residents alike in our restaurants, bars, coffee shops, and at the beach. There will always be a larger than acceptable percentage of our visitors, and even our own residents, who will just not wear them regardless of our laws.
It’s akin to expecting zero objectors to the upcoming coronavirus vaccinations; there will always be persons who decline.
To put it as succinctly as possible — Hawaii is very far from following international scientific consensus. Hawaii leaders, from both the economic and public health sector, must come together to reinstitute some length of quarantine for visitors and returning residents that strikes a better balance between public and economic safety.
Below is a much more accurate calculation of how many infectious visitors will be released into the community by a 72hr pre-travel test + second test system, listed by length of quarantine. Note that the mainland United States is approaching a 1–1.5 percent prevalence rate currently (right column).
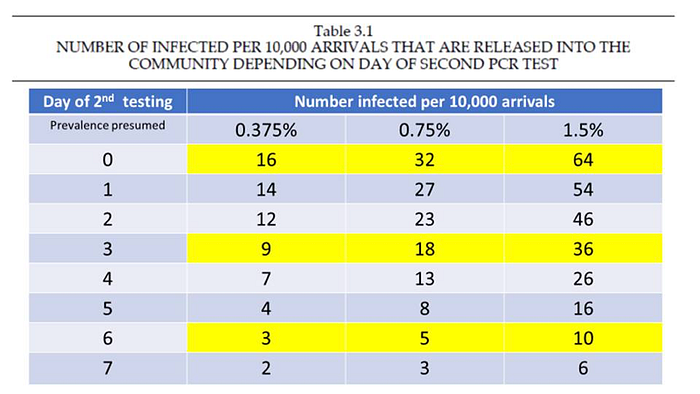
A seven day quarantine, like Vermont has instituted, would be the safest of the above options from a public health perspective. Iceland, which also has a large tourist economy, has opted for five days of quarantine; as did the Commonwealth of the Northern Marianas Islands shown in step 8. New York State has instituted four days. Even the CDC is advising Americans to avoid travel, and many states are suggesting 14 days of quarantine for all who do. Dr Janet Berreman, the Kauai District Health Officer, has also urged Hawaii to temporarily return to a mandatory 14 day quarantine in this November 24th editorial.
The above governments and organizations realize controlling spread requires not only mask use, but a robust screening and prevention fence.
If Hawaii doesn’t do something similar, with at least four to six months to go before 50–70 percent of the population is vaccinated to achieve some semblance of herd immunity, cases will continue to rise, travel linked cases will seed community spread, tiers will go in the opposite direction, our medical capacity will be surpassed, and most importantly, lives will be lost.
Finally, a safer Hawaii will be more attractive to visitors than an unsafe one, and entice longer term vacations. At minimum, if our leadership decides to continue with a one-step plan, there should be transparency regarding the risks.
12. Last but Not Least, Other Very Important Measures To not Forget
- When feasible, please have get-togethers outside, this virus thrives indoors. Thanksgiving should be done outside — if can.
- Do not gather in large groups, especially avoid mixing households.
- Wash your hands.
- Watch your distance to at least six feet.
Me Ke Aloha Pumehana & dul le sláinte,
Darragh Cormac O’Carroll M.D.
Special thanks to Chad Taniguchi J.D. and all involved for their dedication and proofreading.
